
The Science of suPAR
suPAR is a biomarker first described in Denmark in the early 1990s and has since been studied in multiple health and research settings.
Research across diverse populations has demonstrated consistent relationships between suPAR levels and potential markers of adverse health outcomes for those experiencing acute health conditions.
Insights from the Century Project: suPAR, a New Biomarker of Aging and Inflammation
The Guggenheim report analyzes and reviews the different factors that can influence our potential longevity and, in particular, our healthspan, defined as the period of time that we live free of any chronic disease.
The suPAR Protein
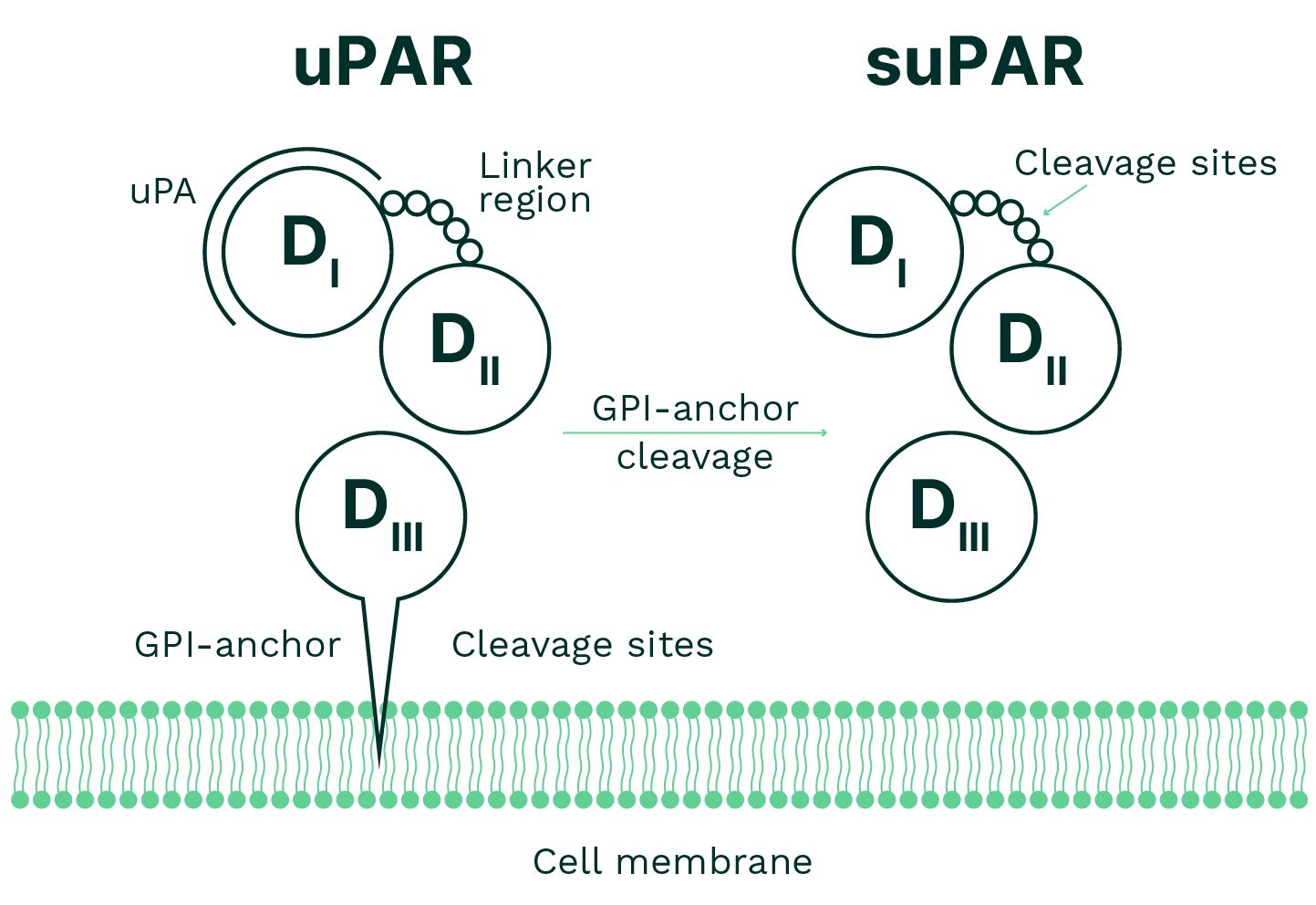
uPAR was originally identified as a receptor for urokinase-type plasminogen activator (uPA), a protein involved in the conversion of plasminogen to plasmin. In addition to binding uPA, uPAR interacts with several proteins and has been studied in cellular processes including migration, adhesion, angiogenesis, proliferation, and chemotaxis. It is expressed on the surface of various cell types, particularly immune cells such as neutrophils, activated T cells, and macrophages, as well as endothelial and smooth muscle cells.
suPAR is the soluble form of uPAR. As illustrated in Figure 1, uPAR is attached to the cell membrane via a glycosylphosphatidylinositol (GPI) anchor. When uPAR is cleaved from the cell surface, it can be released into the circulation as suPAR. Circulating suPAR has been described in research studies in relation to immune and inflammatory processes.
The information above describes findings from scientific literature and is provided for educational purposes only. The suPAR test is not intended to diagnose, treat, or predict disease.
The History of suPAR
First identified in 1991 in research related to cancer progression, suPAR has since been studied extensively in a wide range of health conditions. Elevated suPAR levels have been reported in association with cardiovascular disease, type 2 diabetes, chronic kidney disease, and other age-related conditions.
The Role of suPAR in Immunity and Patient Prognosis
The crystal structure of suPAR was elucidated in 2006 and published in the journal Science, demonstrating that its three-domain structure can rotate around its central axis, allowing interactions with multiple complex ligands. This structural flexibility enables suPAR to maintain a versatile binding pocket, crucial for its involvement in a wide array of biological processes.
uPAR is expressed primarily on the surfaces of immune cells including monocytes and activated T-cells. It plays a role in several immune-related mechanisms such as cell migration, adhesion, angiogenesis, fibrinolysis, and proliferation. When uPAR is cleaved from the cell surface it circulates in soluble form, known as suPAR.
uPAR is involved in processes that localize proteolytic activity at the cell surface. It contributes to the regulation of pericellular proteolysis, which has been studied in contexts such as cell migration and tissue remodeling, including in inflammatory and neoplastic conditions. In its soluble form, suPAR has been shown in research settings to interact with cellular receptors and participate in signaling pathways associated with chemotaxis and immune activity.
Current research suggests that persistently elevated suPAR levels are more commonly associated with ongoing immune activation than inherited genetic differences. Studies have not identified specific genetic variants that inherently cause high suPAR levels in humans. Elevated suPAR levels have been reported across a range of infectious and chronic conditions and, in multiple clinical studies, have been associated with less favorable health outcomes.